
- (212) 621-7746
- text us
- BOOK ONLINE Same Day Appointments
Lower back pain affects women differently than men, and the reasons go beyond general wear and tear. Hormonal fluctuations, pregnancy, pelvic anatomy, and conditions like endometriosis create an entirely separate category of back pain causes that generic articles fail to address. At Sports Pain Management NYC, Dr. Melepura evaluates women with lower back pain daily and finds that the cause, the appropriate diagnostic approach, and the most effective treatment all depend heavily on the patient’s age, hormonal status, and lifestyle.

This guide covers the most common causes of lower back pain in women organized by life stage, explains how to distinguish spinal pain from referred gynecological pain, and introduces the interventional treatments that most women do not know exist.
Women experience lower back pain at higher rates than men throughout their lives, and several anatomical and hormonal factors explain why.
The female pelvis is wider and more tilted than the male pelvis, which shifts the center of gravity forward and increases the curve of the lumbar spine (lordosis). This structural difference places more compressive load on the lower lumbar discs and facet joints. The wider pelvis also changes the angle of the sacroiliac (SI) joints, making them more mobile and more vulnerable to dysfunction, particularly during and after pregnancy.
Estrogen and progesterone directly influence ligament laxity, pain sensitivity, and inflammatory responses. During the premenstrual and menstrual phases, prostaglandin release causes uterine contractions that radiate pain to the lower back. During perimenopause and menopause, declining estrogen accelerates disc degeneration and bone density loss. These hormonal effects mean that a woman’s lower back pain can change character and intensity across her menstrual cycle, through pregnancy, and into menopause.
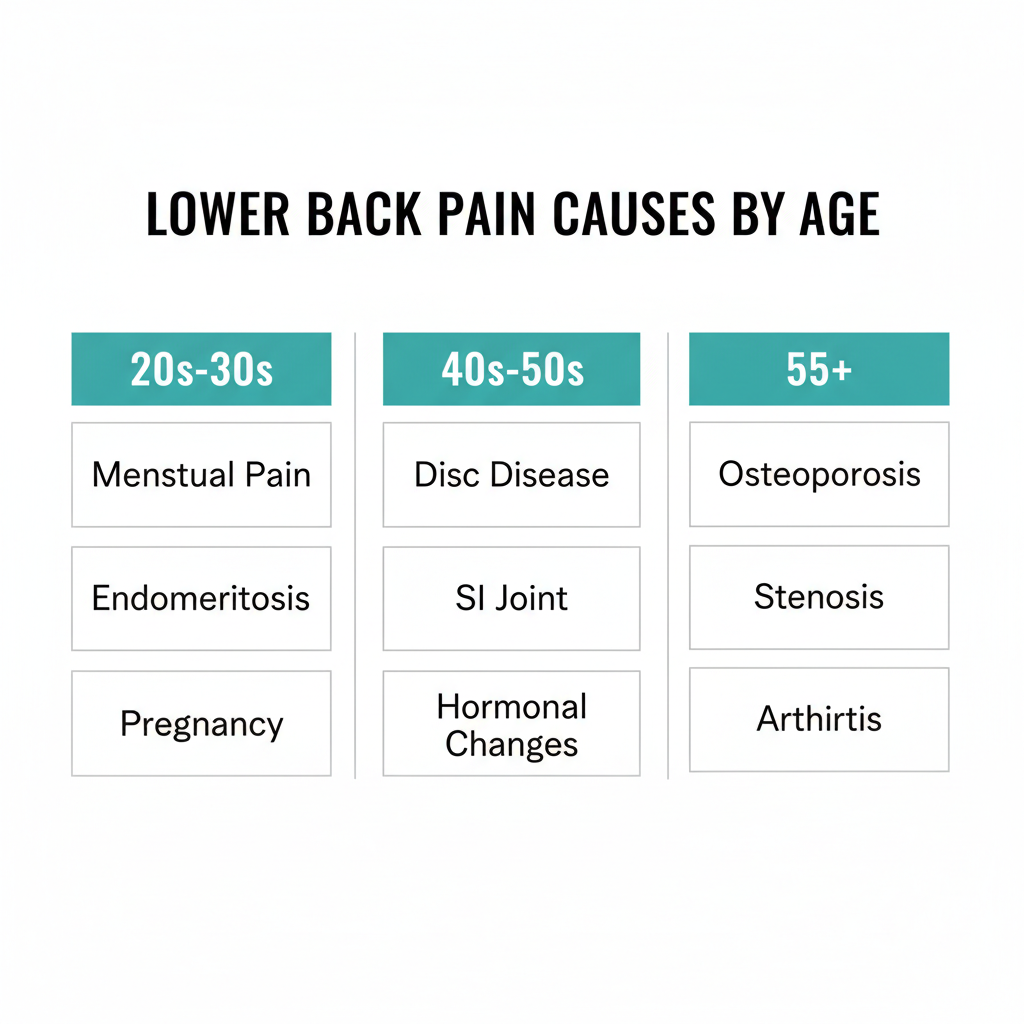
Dysmenorrhea (painful periods) is the most common cause of cyclical lower back pain in younger women. Prostaglandins trigger uterine muscle contractions that refer pain to the lower back and thighs. This pain typically begins 1 to 2 days before menstruation and resolves within 2 to 3 days. PMS and PMDD can produce lower back pain that starts up to a week before the period along with bloating, fatigue, and mood changes.
If your lower back pain follows your menstrual cycle like clockwork, the cause is likely hormonal rather than structural. However, if menstrual back pain is severe enough to interfere with work or daily activities, evaluation for endometriosis is warranted.
Endometriosis affects roughly 10 percent of women of reproductive age and commonly causes lower back pain that is misattributed to muscle strain or poor posture for years before diagnosis. The condition occurs when tissue similar to the uterine lining grows outside the uterus, often on the ligaments supporting the pelvis and spine. Endometriosis-related back pain tends to be worst during menstruation but can become constant as the condition progresses.
The key differentiator: if your lower back pain worsens significantly during your period, is accompanied by pelvic pain or painful intercourse, and has not responded to standard back pain treatments, discuss endometriosis screening with your gynecologist. This is a condition where the back pain is referred from the pelvis, not originating from the spine, and spinal treatments alone will not resolve it.
Up to 70 percent of women experience lower back pain during pregnancy, driven by weight gain, shifted center of gravity, hormonal ligament laxity, and the physical demands of carrying additional weight in the front of the body. Postpartum back pain persists in 30 to 40 percent of women, particularly those who had cesarean deliveries, epidurals, or diastasis recti (abdominal muscle separation).
Postpartum back pain that persists beyond 3 months should be evaluated rather than dismissed as “normal.” SI joint dysfunction, disc problems, and pelvic floor weakness are all treatable causes that can be identified through a specialist evaluation.
Prolonged sitting weakens the core stabilizers and tightens the hip flexors, both of which increase lumbar stress. For women in New York City who commute on the subway (standing on moving trains stresses the spine differently than sitting), work 8 to 10 hours at a desk, and then try to fit in exercise, the cumulative load on the lower back is significant. Add carrying heavy bags on one shoulder and walking in unsupportive footwear, and the mechanical cause becomes clear.
The perimenopausal transition brings fluctuating and declining estrogen levels that directly affect spinal structures. Estrogen helps maintain disc hydration, cartilage integrity, and bone density. As levels drop, discs lose height and cushioning, facet joints develop arthritis changes, and the supporting ligaments become less resilient. Research published in the National Library of Medicine found that women with BMI above 30 during perimenopause have significantly higher rates of lower back pain.
Disc degeneration accelerates after 40, particularly in women due to the estrogen-related changes described above. Symptoms include a deep, aching pain in the lower back that worsens with prolonged sitting and improves with movement. The pain may radiate into the buttocks but typically does not extend below the knee unless a disc is compressing a nerve root.
The sacroiliac joint connects the spine to the pelvis and is a common source of lower back pain in women, particularly after pregnancy and during perimenopause. SI joint dysfunction produces pain in the lower back and buttock on one side, often worsening with prolonged standing, stair climbing, or transitioning from sitting to standing. Women are more susceptible because of wider pelvis geometry, ligament laxity from pregnancy, and hormonal changes that affect joint stability.
SI joint dysfunction is frequently misdiagnosed as a disc problem or sciatica. The critical diagnostic tool is a diagnostic SI joint injection: if injecting local anesthetic into the SI joint eliminates the pain, the diagnosis is confirmed and targeted treatment can proceed.
The piriformis muscle runs from the sacrum to the hip and sits directly over the sciatic nerve. When this muscle is tight or inflamed, it compresses the nerve and produces pain in the lower back, buttock, and down the back of the leg. Women are more likely to develop piriformis syndrome due to wider pelvis angles that increase the muscle’s tension. It is commonly mistaken for sciatica from a disc herniation, but the treatment is different.
Osteoporosis affects approximately 1 in 4 women over 65 and is the leading cause of vertebral compression fractures. These fractures can occur with minimal trauma — bending to pick something up, a minor fall, or even a strong cough. The pain is typically sudden, sharp, and localized to a specific area of the spine. Many compression fractures are initially dismissed as “muscle spasms” because patients do not recall a significant injury.
For painful compression fractures that do not respond to conservative care, minimally invasive procedures like vertebroplasty and kyphoplasty can stabilize the fracture and provide significant pain relief. These are performed as outpatient procedures with rapid recovery.
Spinal stenosis, the narrowing of the spinal canal that compresses the nerves, becomes increasingly common after 55. The hallmark symptom is pain and heaviness in the lower back and legs that worsens with walking and standing but improves with sitting or bending forward (such as leaning on a shopping cart). Women with stenosis often report that they can walk further when pushing a cart than walking upright.
Arthritis of the facet joints in the lumbar spine produces stiffness and pain that is worst in the morning, improves with gentle activity, and returns with prolonged standing or extension (arching the back). Post-menopausal women are particularly susceptible due to years of estrogen decline affecting cartilage integrity. Facet joint injections and medial branch nerve blocks are highly effective treatments for this condition.
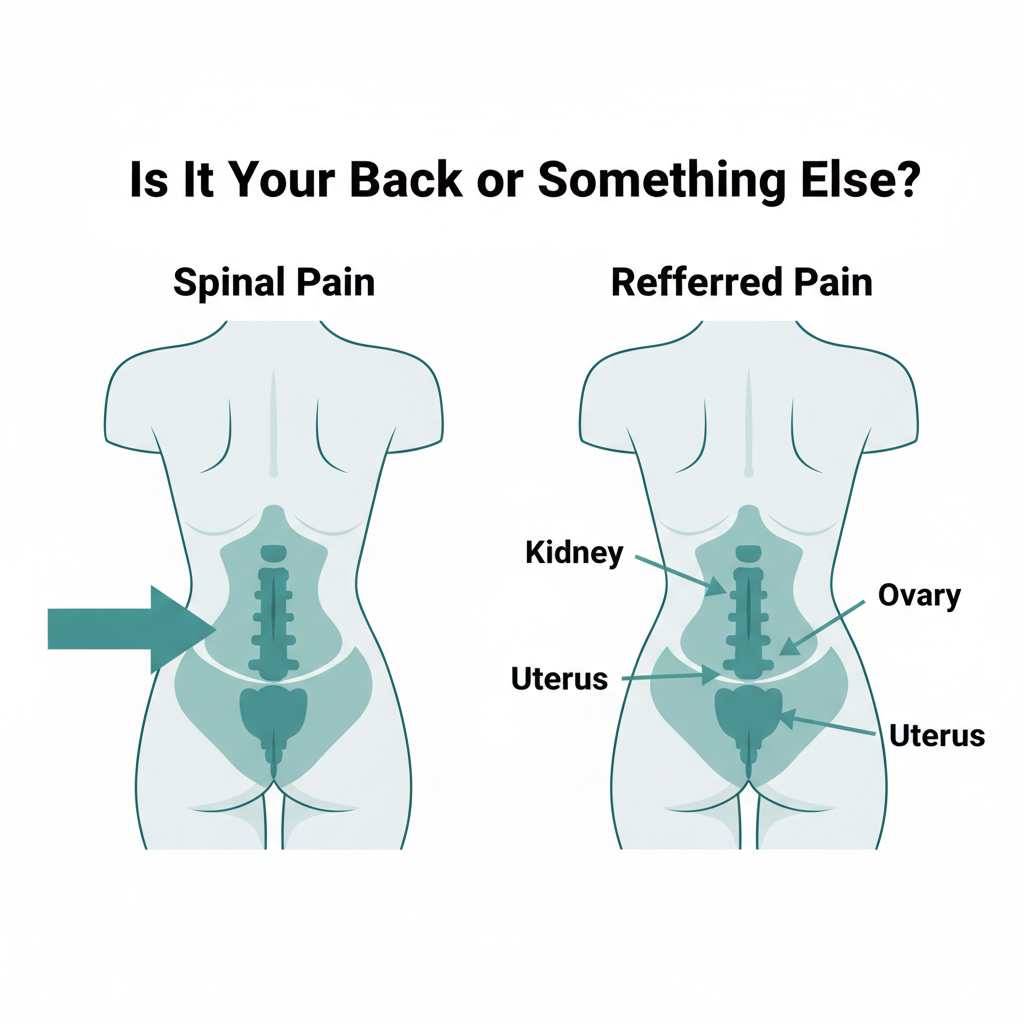
One of the most common sources of confusion for women with lower back pain is whether the pain is actually coming from the spine or being referred from another organ. Several conditions mimic spinal pain:
Kidney pain vs. back pain: Kidney pain is typically felt higher (at the flank, just below the ribs), is often one-sided, and may be accompanied by fever, painful urination, or blood in the urine. Spinal lower back pain is usually centered at the belt line or below and changes with movement and position. If you have lower back pain with urinary symptoms or fever, seek medical evaluation promptly.
Pelvic floor dysfunction: Weakness or tension in the pelvic floor muscles can refer pain to the lower back, sacrum, and tailbone. This is particularly common in postpartum women and women approaching menopause. Pelvic floor physical therapy is the primary treatment.
Ovarian cysts and fibroids: Large ovarian cysts can produce lower back and pelvic pain, particularly if they rupture or twist (ovarian torsion, which requires emergency care). Uterine fibroids, especially those growing toward the back of the uterus, can press on spinal nerves and cause chronic lower back pain.
The advice to “take ibuprofen and stretch” is not a treatment plan. When lower back pain persists beyond 2 to 3 weeks or significantly limits daily function, targeted treatment based on an accurate diagnosis produces far better outcomes than generic self-care.
At Sports Pain Management NYC, Dr. Melepura’s evaluation for women’s lower back pain includes a physical examination with specific provocative tests for SI joint dysfunction, piriformis syndrome, and facet joint involvement. Imaging (X-ray and MRI) evaluates disc health, bone density, and nerve compression. When the diagnosis is unclear, diagnostic injections using image guidance can pinpoint the exact pain source — if injecting a specific joint or nerve eliminates the pain, the source is confirmed.

Modern interventional pain management offers women targeted relief that goes far beyond medication:
All of these procedures are performed in-office or outpatient, typically in 30 minutes or less, with minimal recovery time.

Prevention strategies that actually work for women’s lower back pain:
Start with your PCP for new-onset back pain that is mild to moderate. See a pain specialist directly if your back pain has lasted longer than 4 weeks without improvement, radiates into your legs, is accompanied by numbness or weakness, or has not responded to physical therapy and medication. A back pain specialist can perform diagnostic procedures and targeted treatments that a PCP’s office is not equipped to provide.
Seek immediate evaluation if you have back pain with numbness in both legs, loss of bladder or bowel control, fever, or unexplained weight loss. Schedule a specialist appointment if pain has persisted beyond 3 to 4 weeks, is getting worse, radiates into your leg, or interferes with sleep. Cyclical pain tied to your menstrual cycle is common but should be evaluated if it is severe enough to limit daily activities.
Sudden lower back pain in women is most commonly caused by an acute muscle spasm, a disc herniation, or an SI joint flare. Less commonly, it can result from a kidney infection, an ovarian cyst rupture, or (in women over 55) a vertebral compression fracture. If the pain is severe, one-sided with urinary symptoms, or you are unable to stand, seek same-day evaluation.
Yes. Endometriosis, ovarian cysts, uterine fibroids, and pelvic inflammatory disease can all produce lower back pain. The distinguishing features are pain that correlates with your menstrual cycle, is accompanied by pelvic symptoms (pain during intercourse, abnormal bleeding, urinary urgency), or has not responded to standard back pain treatments. If these apply, gynecological evaluation alongside spinal assessment is important.
The best treatment depends entirely on the specific cause. SI joint dysfunction responds to SI joint injections and potentially radiofrequency ablation. Disc-related pain responds to epidural steroid injections. Facet arthritis responds to medial branch blocks and ablation. Compression fractures respond to vertebroplasty. The common thread is accurate diagnosis first, then targeted treatment — not a generic approach applied to every patient.
For many women, yes. Declining estrogen levels during menopause accelerate disc degeneration, reduce bone density, and increase the risk of facet joint arthritis and compression fractures. Women who were physically active and maintained bone density through resistance training experience less menopausal back pain. For those who develop new or worsening back pain during menopause, early evaluation and treatment prevent progression.
If lower back pain is limiting your work, exercise, or daily life, Dr. Melepura at Sports Pain Management NYC can determine whether the cause is spinal, hormonal, or referred, and build a treatment plan that addresses the specific source. Our Manhattan office offers same-day appointments and advanced diagnostic imaging. Schedule your evaluation here.

Febin Melepura, MD is a top rated, best in class interventional pain management doctor. He is a nationally recognized pain relief specialist and is among the top pain care doctors in New York City and the country. He is an award winning expert and contributor to a prominent media outlets.
Dr. Febin Melepura has been recognized for his thoughtful, thorough, modern approach to treating chronic pain and, among other accolades, has been named a “top pain management doctor in New York”, and one of “America’s Top Doctors™” for an advanced sports injury treatments.
