
- (212) 621-7746
- text us
- BOOK ONLINE Same Day Appointments
Knee pain after running is rarely caused by running itself. It is caused by how you run, how much you run, what you run on, and which muscles are too weak to support the forces your knee absorbs with every stride. The average runner’s knee absorbs 2 to 3 times their bodyweight with each foot strike, multiplied by 1,500 to 2,000 strides per mile. When gait faults, training errors, or muscle imbalances are present, that force concentrates on structures that were not designed to handle it repeatedly.

This guide is written specifically for runners, not general gym-goers. If you are also experiencing knee pain from squats, leg press, or other gym activities, see our companion article on knee pain after working out. This article covers the biomechanical causes specific to running, how to identify which running injury you have based on pain location, when to modify training versus when to stop, and the treatment options that exist between rest and surgery that most runners never hear about.
“Overuse” is not a diagnosis. It is a description of what happened without explaining why. Two runners logging identical mileage can have completely different outcomes because the real determinants of running-related knee pain are biomechanical, not volumetric.
Three gait patterns are responsible for the majority of running knee injuries:
The 10 percent rule (never increase weekly mileage by more than 10 percent) is a useful guideline but incomplete. Intensity matters as much as volume. Adding hill repeats, speed intervals, or tempo runs introduces forces that tendons and cartilage have not adapted to, even if total mileage stays flat. The most common pattern Dr. Melepura sees at our NYC practice is a runner who kept mileage steady but added two speed sessions per week and developed patellar tendonitis within a month.
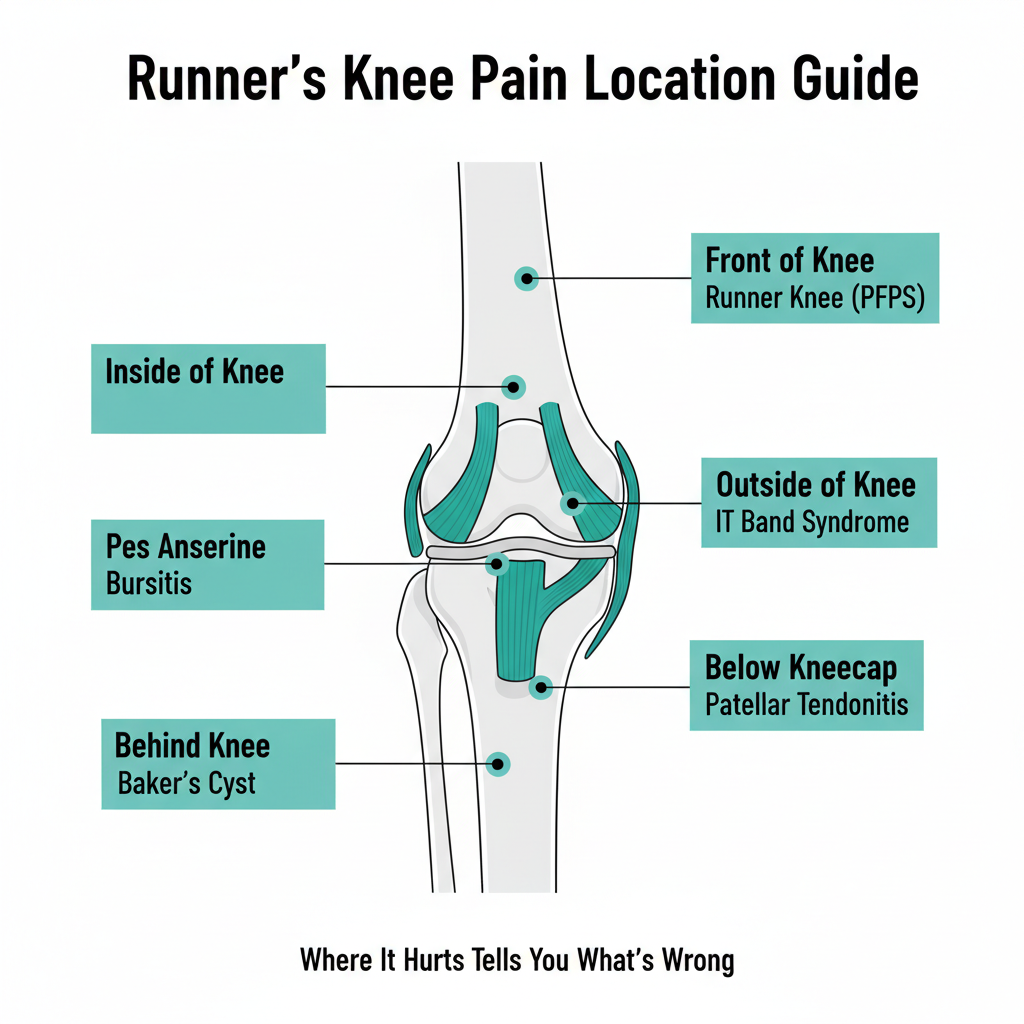
Pain location is the fastest way to narrow down your running injury. Use this guide to identify what you are likely dealing with.
Pain location: Around or behind the kneecap. When it hurts: During and after running, going down stairs, sitting with bent knees for extended periods (“movie theater sign”).
Runner’s knee is the most common running injury, accounting for 25 to 30 percent of all running-related knee pain. The kneecap is not tracking properly in its groove during the repetitive bending motion of running, creating friction and irritation. The primary drivers are weak quadriceps (specifically the VMO, the inner quad muscle), weak hip stabilizers, and tight IT bands that pull the kneecap laterally.
The critical point for runners: runner’s knee responds to targeted strengthening, not just rest. Taking two weeks off and then returning to the same mileage without addressing the underlying weakness produces the same outcome. Single-leg squats, step-downs, and hip abduction exercises performed 3 times per week while maintaining low-impact cross-training resolve most cases in 6 to 8 weeks.
Pain location: Outside of the knee, specifically over the lateral femoral epicondyle (the bony prominence on the outer knee). When it hurts: Usually starts 10 to 15 minutes into a run at a consistent distance, worsens with downhill running. See our IT band syndrome page for detailed information.
The IT band is a thick strip of connective tissue running from the hip to just below the knee. In runners, it becomes irritated where it crosses the outer knee during the repetitive bending cycle. IT band syndrome is the second most common running injury and is strongly associated with three factors: rapid mileage increases, running on cambered surfaces (sloped roads, banked tracks), and weak hip abductors.
NYC runners face additional IT band risk from Central Park loop running. The main loop road has a consistent camber (slope toward the curb for water drainage) that applies asymmetric stress to the downhill knee. Alternating direction around the park or using the flatter bridle path reduces this exposure.
Pain location: Below the kneecap, at the top of the shinbone. When it hurts: During running (especially hills and speed work), jumping, going down stairs.
Patellar tendonitis is a repetitive strain injury of the tendon connecting the kneecap to the shinbone. Runners who add hill work, speed intervals, or trail running without adequate progression are the most common patients. The hallmark pattern is pain that appears during warmup, temporarily improves as the tendon warms up mid-run, then returns worse afterward and the next morning.
Pain location: Along the joint line, inner or outer edge of the knee. When it hurts: With twisting, pivoting, deep squatting. May include clicking or locking.
Pure straight-line running does not commonly cause meniscus tears, but trail running with uneven surfaces, running with sudden direction changes, and running on a degenerative meniscus (common in runners over 35) can produce tears. The distinguishing feature is mechanical symptoms: catching, clicking, or the knee locking in a bent position. If your knee pain is accompanied by these symptoms, imaging with MRI is warranted. Learn more on our knee pain page.
Pain location: Inner side of the knee, about 2 inches below the joint line. When it hurts: After running, going up stairs, at night when lying with knees together.
The pes anserine bursa sits where three tendons insert on the inner tibia. It becomes inflamed in runners with tight hamstrings, excessive pronation, or who suddenly increase hill running. It is frequently misdiagnosed as a medial meniscus tear because the pain location overlaps. The distinction matters: bursitis responds quickly to anti-inflammatory treatment and often a single corticosteroid injection, while a meniscus tear may need a different approach. Visit our knee bursitis page for more.
Pain location: Inner side of the kneecap. When it hurts: Snapping or catching sensation during bending, may produce a palpable band along the inner kneecap.
Plica syndrome is one of the most underdiagnosed causes of knee pain in runners. The plica is a fold of synovial tissue inside the knee that can become thickened and irritated from repetitive bending. It mimics runner’s knee and meniscus symptoms, which is why many runners try treatments that do not work before getting the correct diagnosis. An experienced physical exam can identify plica syndrome without imaging.
Many runners experience a confusing pattern: the knee feels fine during the run but hurts afterward, sometimes not appearing until several hours later or the next morning. This delayed onset usually indicates an inflammatory response rather than a structural failure, and is common with early-stage runner’s knee, patellar tendonitis, and IT band irritation.
During running, increased blood flow and endorphins mask the pain signal. After cooling down, the inflammatory cascade catches up. This pattern is your body telling you that the tissue is being stressed beyond its current tolerance. It does not mean you need to stop running entirely, but it does mean your training load has outpaced your tissue capacity and modification is needed.

Running surface affects impact force more than most runners realize:
For NYC runners dealing with knee pain, the single most impactful change is switching some or all runs to Central Park’s bridle path or the soft-surface trails in Prospect Park, Riverside Park, or the Bronx’s Van Cortlandt Park (which has a famous cross-country course).
Shoe choice affects knee load through three variables:
Replace running shoes every 300 to 500 miles regardless of how they look. Midsole cushioning degrades before the outsole shows wear.
Use this framework to decide whether to run, modify, or stop:
Safe to run with modifications: Pain is mild (1 to 3 out of 10), appears only after the run, resolves within 24 hours, and is not worsening week to week. Reduce mileage by 20 to 30 percent and avoid hills and speed work.
Modify to cross-training: Pain is moderate (4 to 6 out of 10), appears during the run but does not alter your gait, and takes 24 to 48 hours to resolve. Switch to cycling, pool running, or swimming while addressing the cause.
Stop running and get evaluated: Pain alters your gait (you are limping or compensating), is present during daily activities like stairs, is accompanied by swelling, clicking, or instability, or has been worsening over 2 or more weeks.
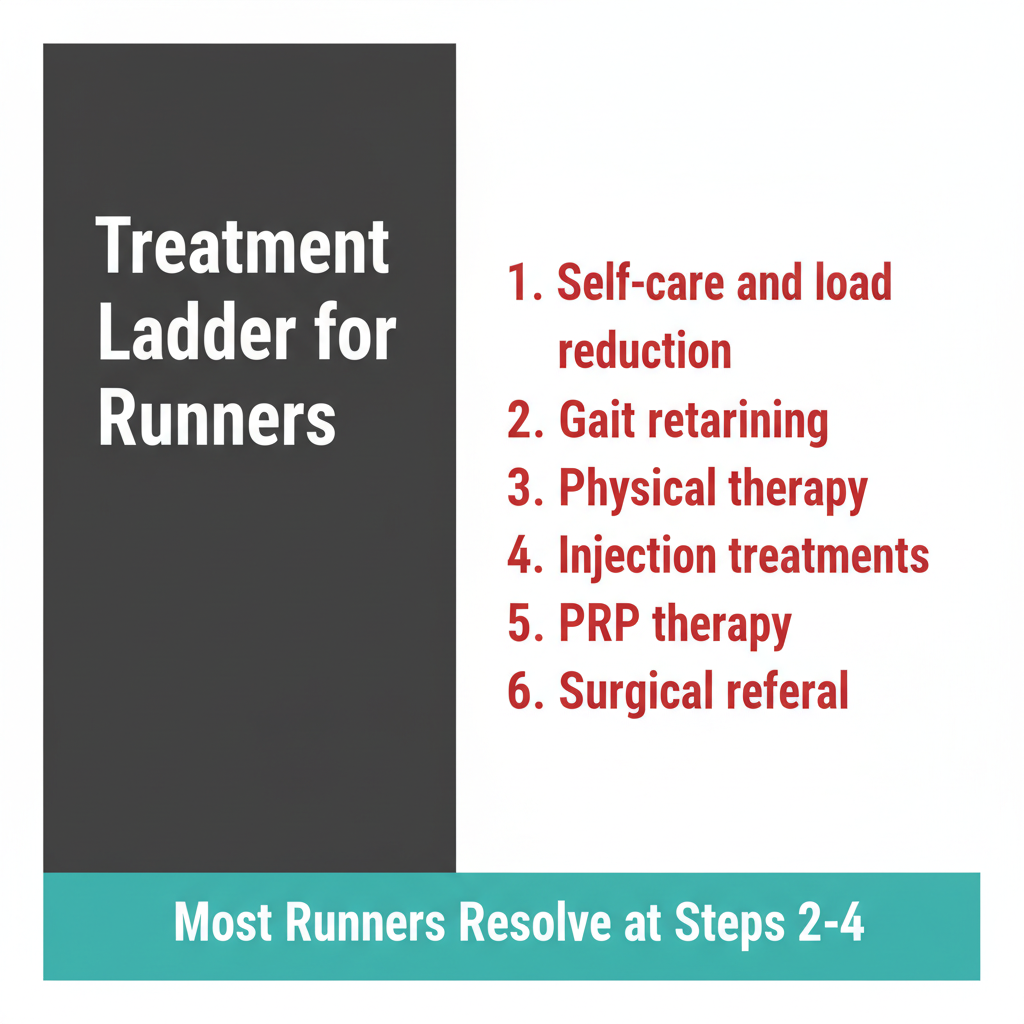
Every running knee pain article online tells you to rest and ice. Here is the complete treatment pathway, including the options between rest and surgery that runners need to know about.
Structured PT targeting the specific diagnosis: quad and VMO strengthening for runner’s knee, hip abductor work for IT band syndrome, eccentric loading for patellar tendonitis. Gait analysis and running form correction address the biomechanical root cause. Running should continue at a reduced load during PT unless the therapist advises otherwise.
When 6 to 8 weeks of PT and training modification have not resolved the pain, interventional treatments offer the next step without surgery:
Most of these procedures take 15 to 30 minutes and require no downtime from daily activities. Return to running follows a structured protocol that Dr. Melepura develops based on your specific diagnosis and treatment response. Learn more on our knee injection treatments page.
Surgery is appropriate for complete ligament tears, large meniscus tears with persistent locking, and structural problems that have not responded to conservative and interventional approaches. The advantage of the treatment ladder approach is that surgery is considered only after all less invasive options have been exhausted, and many runners find their solution at Level 2 or 3.

Prevention is strength, not stretching. The single most effective intervention for preventing running knee injuries is a targeted hip and quad strengthening program performed 2 to 3 times per week alongside your running.
For runner-specific knee exercise protocols you can start today, visit our knee exercises page.
Running in New York City comes with specific challenges that affect knee health:
Sometimes, but only if the root cause is addressed. Resting for two weeks and then returning to the same training with the same muscle imbalances produces the same outcome. Runner’s knee resolves reliably with targeted hip and quad strengthening combined with running form correction. Most cases improve within 6 to 8 weeks of consistent rehab work.
Mild pain (1 to 3 out of 10) that appears only after running, resolves within 24 hours, and is not worsening is generally safe to run through with reduced volume. Stop running if the pain changes your gait, is present during daily activities, or is accompanied by swelling or instability. Cross-training (cycling, swimming, pool running) maintains fitness while the knee recovers.
Common, but not normal. Knee pain after a 5K in a beginner runner usually indicates that training volume increased faster than the tissues adapted. In an experienced runner, it suggests a biomechanical issue or the beginning of a structural problem. Either way, it warrants attention rather than dismissal. Start with the prevention exercises above and see a specialist if pain persists beyond 2 to 3 weeks.
Runner’s knee produces a dull, diffuse ache around the kneecap that worsens with stairs, prolonged sitting, and running. Meniscus tears produce joint line pain (inner or outer edge of the knee), clicking or catching during bending, and sometimes a locking sensation where the knee cannot fully straighten. Runner’s knee responds to strengthening exercises within weeks. Meniscus symptoms that include mechanical catching or locking need imaging evaluation.
With proper treatment (not just rest), runner’s knee typically improves significantly within 4 to 6 weeks and resolves fully within 8 to 12 weeks. The timeline depends on severity, how long the condition has been present, and adherence to strengthening exercises. Runners who continue targeted PT exercises as maintenance after recovery have significantly lower recurrence rates.
Yes, in most cases. Walking maintains blood flow, prevents stiffness, and provides a low-load stimulus that supports healing. The exception is if walking produces significant pain (above 3 out of 10) or causes a limp. Use walking as active recovery on rest days and as a running substitute during the acute phase.
If knee pain is cutting your runs short or keeping you off the road entirely, Dr. Melepura at Sports Pain Management NYC can identify the specific cause and build a treatment plan that gets you running again. Our Manhattan practice offers same-day appointments, in-office diagnostic imaging, and the full range of non-surgical treatments from targeted injections to regenerative therapies. Schedule your evaluation here.

Febin Melepura, MD is a top rated, best in class interventional pain management doctor. He is a nationally recognized pain relief specialist and is among the top pain care doctors in New York City and the country. He is an award winning expert and contributor to a prominent media outlets.
Dr. Febin Melepura has been recognized for his thoughtful, thorough, modern approach to treating chronic pain and, among other accolades, has been named a “top pain management doctor in New York”, and one of “America’s Top Doctors™” for an advanced sports injury treatments.
