
The most common knee injuries from running are runner's knee (patellofemoral pain syndrome), IT band syndrome, patellar tendinitis, meniscus tears, chondromalacia patella, and stress fractures near the knee. Most are overuse injuries that build up from repetitive load rather than one dramatic moment, and most respond well to non-surgical care when caught early. If you run in New York City, the loops in Central Park, the hard pavement on the avenues, and a marathon training block that ramps up too fast are all common triggers. This guide covers what each injury is, where it tends to hurt, why running causes it, and when knee pain means it is time to have a specialist look.
This article helps you understand what your knee pain might be. It is not a diagnosis, and knee pain that locks, gives way, or will not settle deserves a real exam.
Key Takeaways
- The six most common running knee injuries are runner's knee, IT band syndrome, patellar tendinitis, meniscus tears, chondromalacia patella, and stress fractures near the knee.
- Most are overuse problems driven by training spikes, weak hips, and hard surfaces, not single accidents.
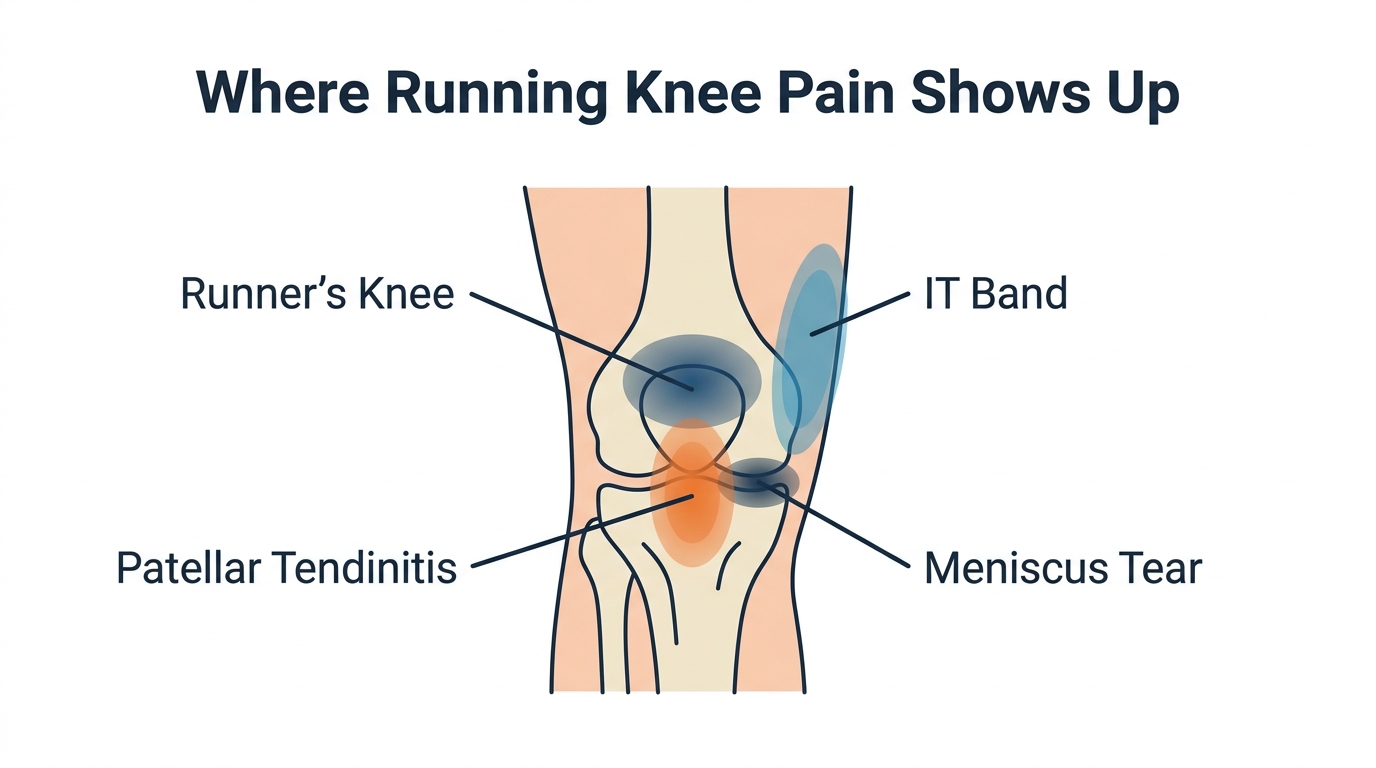
- Runner's knee causes diffuse pain around the kneecap that worsens on stairs and after sitting; a meniscus tear causes sharper joint-line pain that may catch or lock. Outside-knee pain points toward IT band syndrome, and pain just below the kneecap toward patellar tendinitis.
- Most of these injuries improve with rest, activity modification, targeted strengthening, and in some cases an image-guided injection, with surgery as a later resort.
- See a doctor if your knee locks, gives way, swells quickly, will not bear weight, or does not improve after about two weeks of rest.
What Causes Most Running Knee Injuries
Most running knee injuries come from cumulative load, not a single accident. Every running step sends force through the knee several times your body weight, and over thousands of repetitions that load finds the weakest link. Weak or tight hip and thigh muscles, sudden jumps in weekly mileage, worn shoes, and repeated impact on concrete all push the knee past what it can absorb. Cleveland Clinic notes that patellofemoral pain often develops gradually from a mix of muscle imbalance, tight muscles, and excessive load from training errors.
New York adds its own stresses. Long stretches of pavement are less forgiving than trails, downhill segments load the outside of the knee, and the classic spring mistake of doubling mileage to chase a fall marathon goal is a reliable way to inflame a tendon. The cause matters, because the fix is about load, mechanics, and recovery, not just resting until the pain fades and repeating the pattern.
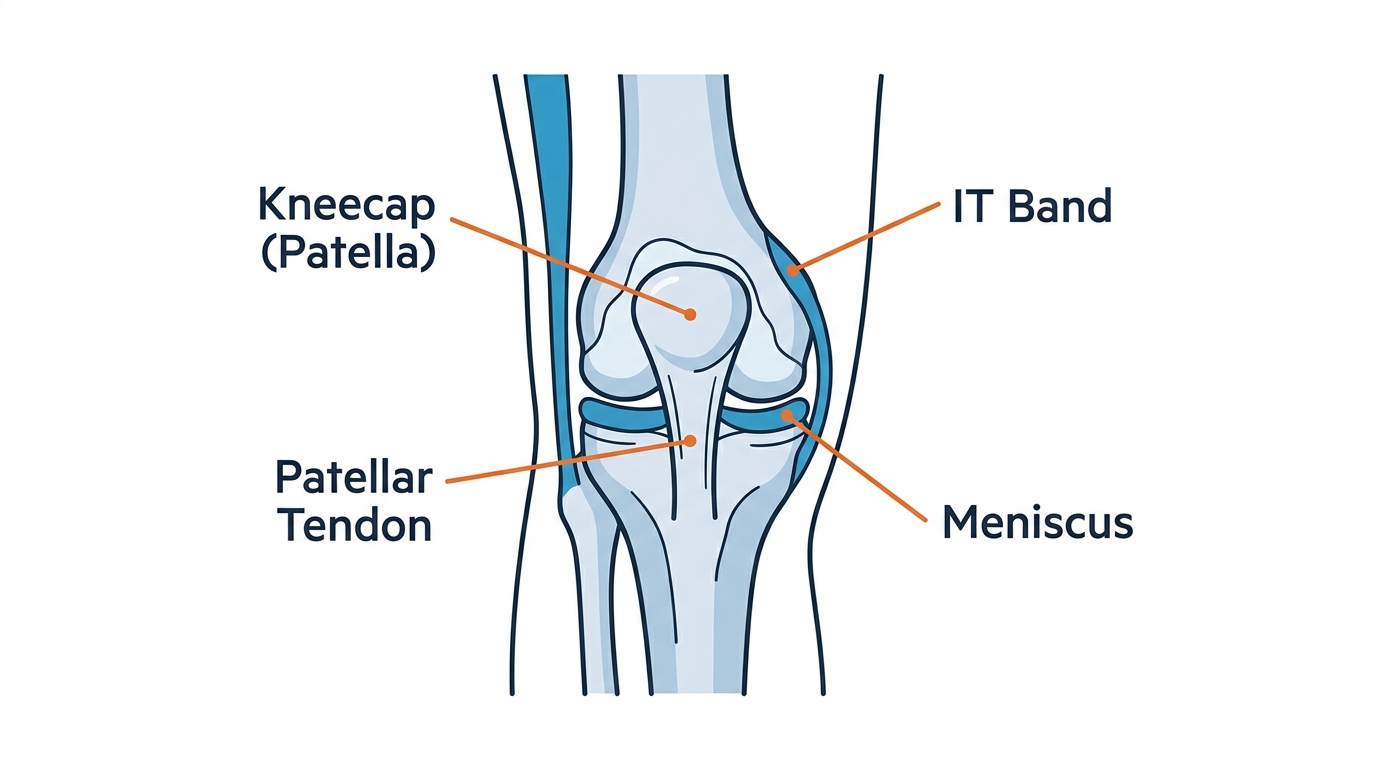
Runner's Knee (Patellofemoral Pain Syndrome)
Runner's knee is pain around or behind the kneecap, and it is the single most common running knee injury. Clinically called patellofemoral pain syndrome, it happens when the kneecap does not track smoothly in its groove as you bend and straighten the leg. The pain is usually a dull ache at the front of the knee, often on both sides of the kneecap, and it can come with a grinding or clicking sensation.
You will typically notice it going up or down stairs, running downhill, squatting, or after sitting with the knee bent for a while, a pattern runners call the movie sign. It builds gradually rather than appearing suddenly. According to Cleveland Clinic , most cases improve within one to two months with non-surgical care.
Treatment is conservative and focuses on the cause: relative rest, hip and quadriceps strengthening, attention to form and mileage, and short-term anti-inflammatory measures. When pain is stubborn, a targeted knee injection can calm the joint enough to let you rebuild strength.
IT Band Syndrome
IT band syndrome causes pain on the outside of the knee and is the most common running injury after runner's knee. The iliotibial band is a thick band of tissue that runs along the outside of the thigh from the hip to just below the knee. With repetitive bending it becomes irritated where it passes the outer knee, producing a sharp or burning pain that often flares partway into a run.
The hallmark is lateral knee pain that gets worse on downhills and when the foot strikes the ground. AAOS OrthoInfo describes IT band syndrome as a friction-driven overuse injury common in runners, and reports that most people recover and return to running within about six weeks using non-surgical care.
Treatment focuses on offloading the irritated tissue and fixing what overloaded it: reducing mileage and downhill volume, hip abductor and glute strengthening, and a gradual return to running. Because the IT band itself is hard to stretch, the lasting fix is strength and load management, not foam rolling alone.
Patellar Tendinitis (Jumper's Knee)
Patellar tendinitis causes pain just below the kneecap, where the patellar tendon connects the kneecap to the shinbone. It is also called jumper's knee because it is common in jumping sports, but runners develop it too, especially with hill repeats, speed work, or a fast jump in intensity. The pain typically starts mild and activity-related, then becomes more constant if you keep training through it.
To localize it, press the soft spot just under the kneecap, which is usually tender with patellar tendinitis. SPIN describes how it approaches patellar tendonitis for runners and jumping athletes. Treatment emphasizes loading the tendon correctly rather than fully resting it, through progressive strengthening, intensity management, and in persistent cases an image-guided injection. Tendons heal slowly, so a graded return matters more than aggressive early mileage.
Meniscus Tears
A meniscus tear causes pain at the joint line, the space between the thigh bone and shin bone, often with swelling and a sense of catching or locking. The meniscus is a C-shaped piece of cartilage that cushions the knee, and in runners a tear usually comes from a twist or pivot, or from gradual wear in older runners. The pain is often sharper than runner's knee and tied to a specific movement.
The telltale features are mechanical: the knee catches, clicks painfully, locks, or feels like it might give way, which points toward cartilage involvement rather than a tracking problem. SPIN explains diagnosis and non-surgical options for a meniscus tear , including when imaging is warranted. Many tears, especially on the outer edge with better blood supply, settle with rest, activity modification, strengthening, and sometimes an injection. Surgery is reserved for tears that lock the knee or fail to respond, so a non-surgical-first evaluation is worthwhile before assuming you need an operation.
Runner's Knee vs Meniscus Tear
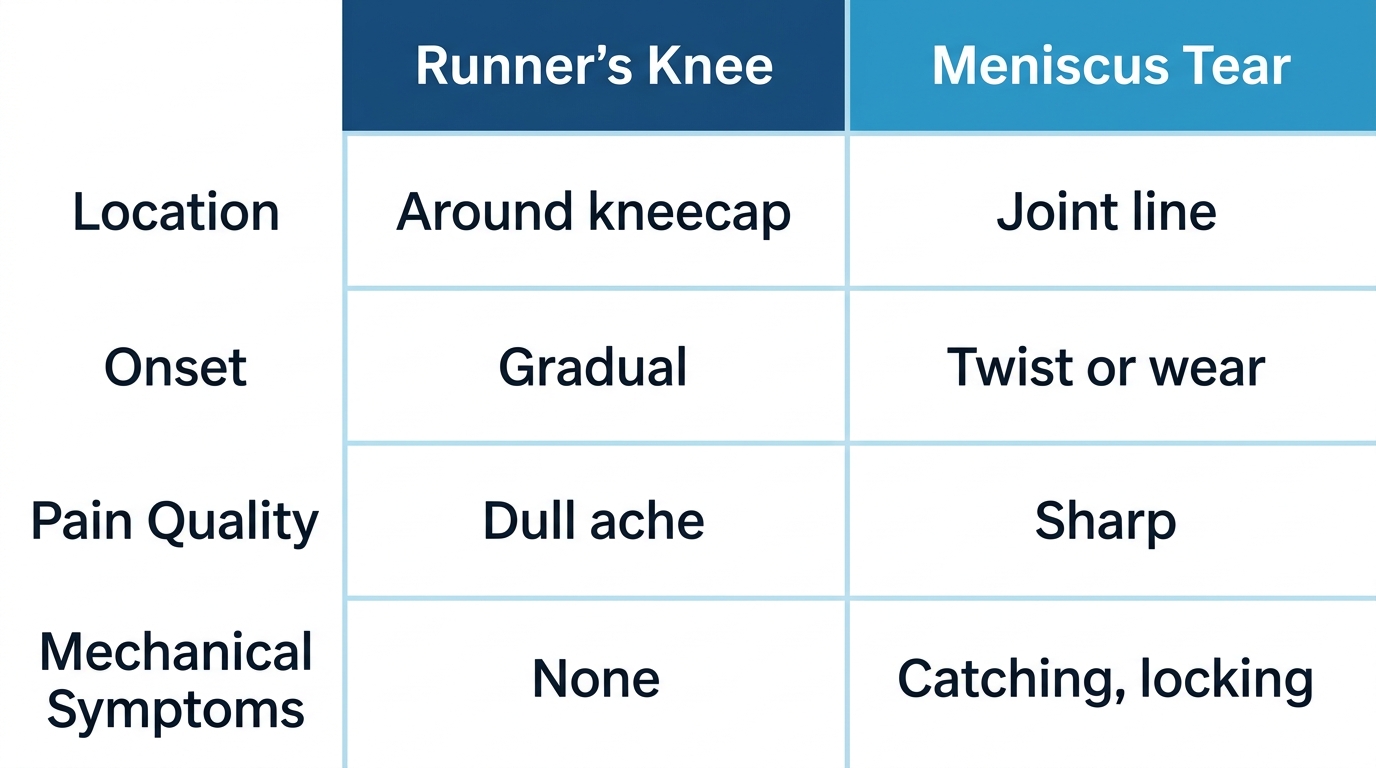
The simplest way to tell runner's knee from a meniscus tear is by where it hurts and whether the knee catches. Runner's knee is diffuse pain around or behind the kneecap; a meniscus tear is sharper pain at the joint line, often with swelling and mechanical symptoms like catching or locking. Here is the side-by-side runners ask about most:
- Location: Runner's knee sits at the front, around the kneecap. A meniscus tear sits at the joint line on the side of the knee.
- Onset: Runner's knee builds slowly from overuse. A meniscus tear follows a twist or pivot, or appears with wear over time.
- Pain quality: Runner's knee is a dull ache tied to load. A meniscus tear is sharper and tied to specific movements.
- Mechanical symptoms: Catching, locking, or the knee giving way suggests a meniscus tear, not runner's knee.
- Aggravators: Runner's knee flares on stairs, downhills, and after sitting. A meniscus tear flares with twisting, deep squatting, and pivoting.
This is a starting point, not a verdict. The two can coexist, and only a hands-on exam plus imaging can confirm which is driving your pain.
Chondromalacia Patella
Chondromalacia patella is the breakdown or softening of the cartilage on the underside of the kneecap, which creates friction and front-of-knee pain. It overlaps with runner's knee, but chondromalacia refers specifically to the cartilage damage itself. Runners feel it as an ache behind the kneecap, sometimes with grinding, that worsens with stairs, squatting, and kneeling.
It tends to show up in runners with repeated high mileage, kneecap tracking problems, or a previous knee injury. SPIN covers symptoms and treatment for chondromalacia patella and how it differs from a simple tracking issue. Treatment is conservative first, built on activity modification, strengthening the muscles that control the kneecap, and managing inflammation, with injections considered when pain limits the rehab itself. Early attention matters because cartilage does not regenerate easily once it is worn.
Stress Fractures Near the Knee
A stress fracture near the knee is a small overuse crack in bone that causes pinpoint pain which worsens with running and eases with rest. Runners develop them in the shin and around the knee after rapid increases in mileage, frequency, or intensity, especially on hard surfaces. The pain often starts after a run, then over time shows up during the run and even with daily walking.
AAOS OrthoInfo describes stress fractures as overuse injuries that occur when fatigued muscles can no longer absorb shock, and stresses that you should not train through the pain. This is one running injury where pushing on makes the problem meaningfully worse. Treatment is rest from impact, a gradual loading plan, and addressing the training error or bone-health factor behind it, and it is the injury most likely to need imaging to confirm.
When to See a Doctor in NYC
See a doctor for running knee pain if it locks, gives way, swells quickly, will not bear weight, or does not improve after about two weeks of rest. These are signs that something more than simple overuse may be going on, and the point where self-care has done its job and a real exam is the next step.
Treat the following as red flags that warrant prompt evaluation:
For active New Yorkers, the practical question is who to see and how fast. A non-surgical interventional pain specialist can examine the knee, order imaging if needed, and treat many of these conditions with physical therapy guidance and image-guided injections before surgery ever enters the conversation. If you are dealing with ongoing knee pain , a clear answer early protects both your training and your long-term joint health.
- The knee locks, catches, or gives way under you.
- A loud pop at the moment of injury, then swelling.
- Rapid or significant swelling, redness, or warmth around the joint.
- Inability to put weight on the leg or straighten the knee.
- Pain that wakes you at night or does not ease with rest.
- Pinpoint bone pain that worsens every time you run.
Preventing Running Knee Injuries and Returning Safely
You prevent most running knee injuries by increasing load gradually, strengthening your hips and thighs, and respecting recovery. Build weekly mileage slowly rather than in big jumps, keep your shoes in reasonable shape, and mix in surfaces softer than concrete when you can. Hip and glute strength work is one of the highest-value habits, since weak hips are a common upstream cause of both runner's knee and IT band syndrome.
Return after pain in stages. Run pain-free in daily life first, then reintroduce easy running at reduced volume, and only add speed or hills once the easy running stays comfortable. If pain returns at the same point each time, the underlying cause has not been addressed, and that is worth an evaluation rather than another cycle of rest and reinjury.

Frequently Asked Questions
Knee pain is more likely serious if the knee locks, gives way, swells quickly, will not bear weight, or does not improve after about two weeks of rest. Pain that wakes you at night or pinpoint bone pain that worsens with every run also warrants an exam. Diffuse aching that eases with rest and improves with reduced mileage is usually a milder overuse problem.
Get Your Knee Checked Before You Train Through It
If your knee pain has lasted more than a couple of weeks or you are noticing any of the warning signs above, you do not have to wait it out or assume surgery is the only path. Dr. Febin Melepura offers same-day evaluations and minimally invasive, non-surgical treatment at his Midtown Manhattan clinic. Schedule a visit to find out what is going on with your knee and what your options are.









