
- (212) 621-7746
- text us
- BOOK ONLINE Same Day Appointments
Knee pain that flares every time you bend or straighten your leg usually points to a specific structural problem, not general wear and tear. The bending and straightening motion loads the meniscus, kneecap, tendons, and ligaments in a precise sequence, and whichever structure is damaged will produce pain at a predictable point in that arc. As a pain management specialist who evaluates this symptom daily at our Manhattan practice, Dr. Melepura finds that most patients can narrow down their likely diagnosis before they even walk into the exam room, simply by paying attention to where and when the pain occurs.

This guide explains the most common causes of knee pain when bending and straightening, how to assess the severity of your symptoms, what happens during a specialist evaluation, and which non-surgical treatments most people do not know exist.
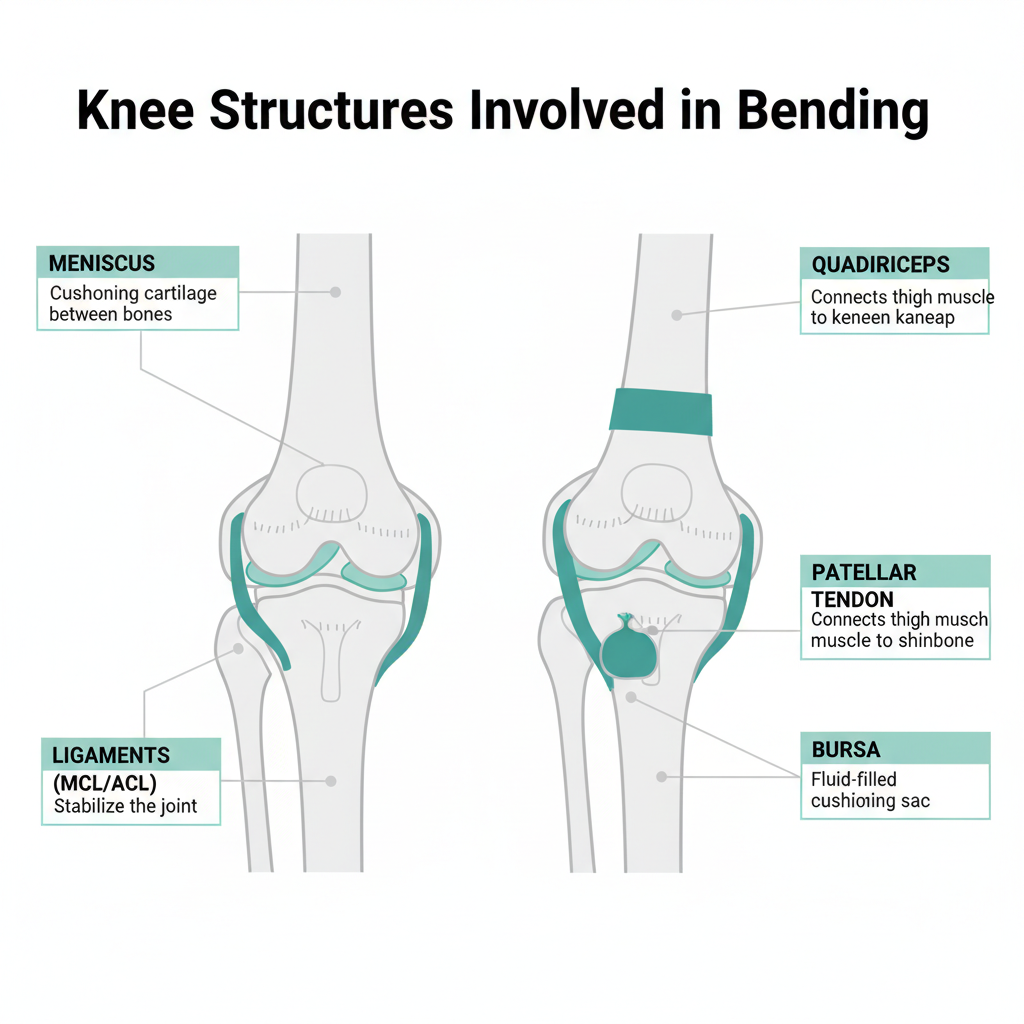
The knee joint relies on cartilage, tendons, ligaments, and a fluid-filled capsule to move through its full range of motion. Bending loads the back of the joint and compresses the meniscus. Straightening loads the front and pulls on the quadriceps tendon and patellar tendon. Pain during one phase, both phases, or at a specific angle tells you which structure is involved.
A meniscus tear is the most common structural cause of pain with bending and straightening. The meniscus is a C-shaped piece of cartilage that cushions the space between the thighbone and shinbone. When torn, it produces catching, clicking, or locking sensations during knee movement.
There are two distinct types. Traumatic tears happen suddenly during a pivot, deep squat, or sports collision and cause immediate pain and swelling. Degenerative tears develop gradually in patients over 35 to 40 and may start as mild stiffness that progresses over weeks. The critical point most articles miss: many degenerative meniscus tears respond well to non-surgical treatment including physical therapy and targeted injections, and do not require arthroscopic surgery.
Runner’s knee produces a dull, aching pain around or behind the kneecap that worsens with bending activities like squatting, climbing stairs, or sitting with bent knees for extended periods. The underlying problem is poor patellar tracking, where the kneecap does not glide smoothly in its groove during movement.
This condition affects far more than just runners. Office workers who sit for 8 or more hours, lifters who squat heavy, and cyclists all develop patellofemoral pain. Weak quadriceps and hip stabilizers are the primary contributors, and targeted strengthening programs resolve the condition in 70 to 90 percent of cases within 6 to 12 weeks.
Pain behind the knee during bending usually indicates one of three problems. A Baker’s cyst is a fluid-filled swelling that forms behind the knee when excess joint fluid accumulates, often secondary to arthritis or a meniscus tear. It causes tightness and pressure that worsens with full bending. Hamstring tendonitis produces pain at the back of the knee where the hamstring tendons insert, particularly during deep bending or running. A posterior meniscus tear causes deep joint line pain that intensifies when the knee bends past 90 degrees.
Baker’s cysts are not dangerous on their own, but they signal an underlying joint problem that needs attention. Draining the cyst provides temporary relief, but the fluid returns unless the root cause is treated.
Sharp, sudden pain during bending is different from a dull ache and narrows the diagnosis significantly. A loose body, which is a fragment of cartilage or bone floating inside the joint, produces intermittent sharp pain that seems to come and go randomly. A meniscus flap tear catches during movement and produces a sharp, stabbing sensation at a specific angle. Plica syndrome, where a fold of the joint lining becomes thickened and irritated, produces a sharp snap or catch on the inner side of the kneecap during bending.
Plica syndrome is one of the most commonly overlooked causes of knee pain in active patients. It mimics meniscus symptoms but does not show up on standard X-rays. Dr. Melepura identifies it through specific physical examination maneuvers and targeted ultrasound when indicated.
Patellar tendonitis causes sharp pain just below the kneecap that flares during bending under load, particularly squatting, jumping, or going down stairs. The patellar tendon connects the kneecap to the shinbone and absorbs enormous force during bending. Athletes who do repetitive jumping, heavy squats, or explosive movements are most susceptible.
The characteristic pattern is pain that appears during warmup, fades mid-activity as the tendon warms up, then returns worse afterward and the following morning. If this matches your experience, reducing training load and starting eccentric strengthening exercises early prevents progression to chronic tendon degeneration.
The knee contains multiple bursae, small fluid-filled sacs that reduce friction between bones, tendons, and muscles. Two types are particularly relevant to bending pain. Prepatellar bursitis causes swelling and tenderness directly over the front of the kneecap and is common in people who kneel frequently. Pes anserine bursitis produces pain on the inner side of the knee about 2 inches below the joint line, worsening with bending and stair climbing.
Pes anserine bursitis is frequently misdiagnosed as a medial meniscus tear because the pain location overlaps. The distinction matters because treatment is different: bursitis responds quickly to anti-inflammatory treatment and sometimes a single corticosteroid injection, while meniscus tears may need a more comprehensive approach. Learn more on our knee bursitis page.
Osteoarthritis causes pain with bending that follows a distinctive pattern: stiffness and pain when you first start moving (morning stiffness lasting 15 to 30 minutes), improvement with gentle activity, then worsening again with prolonged use. The joint may feel gritty or produce a grinding sensation during bending.
Over 14 million Americans have symptomatic knee osteoarthritis, and the condition is most common in adults over 45 with a history of athletic activity or previous knee injuries. The important point for patients to understand is that arthritis does not automatically mean surgery. Modern treatments including viscosupplementation (hyaluronic acid injections), PRP therapy, and genicular nerve blocks provide significant relief and can delay or prevent joint replacement in many cases.
Ligament injuries produce pain with bending that is accompanied by a feeling of instability, as though the knee might give way. An ACL tear typically involves a distinct popping sensation at the time of injury followed by rapid swelling. MCL sprains cause pain on the inner side of the knee that worsens with bending and any twisting motion.
Grade 1 MCL sprains resolve with bracing and rest in 2 to 4 weeks. Complete ACL tears in active patients often require surgical reconstruction, but partial tears and lower-demand patients may be candidates for non-surgical management with structured rehabilitation. Visit our sprained knee page for more on ligament injury evaluation.
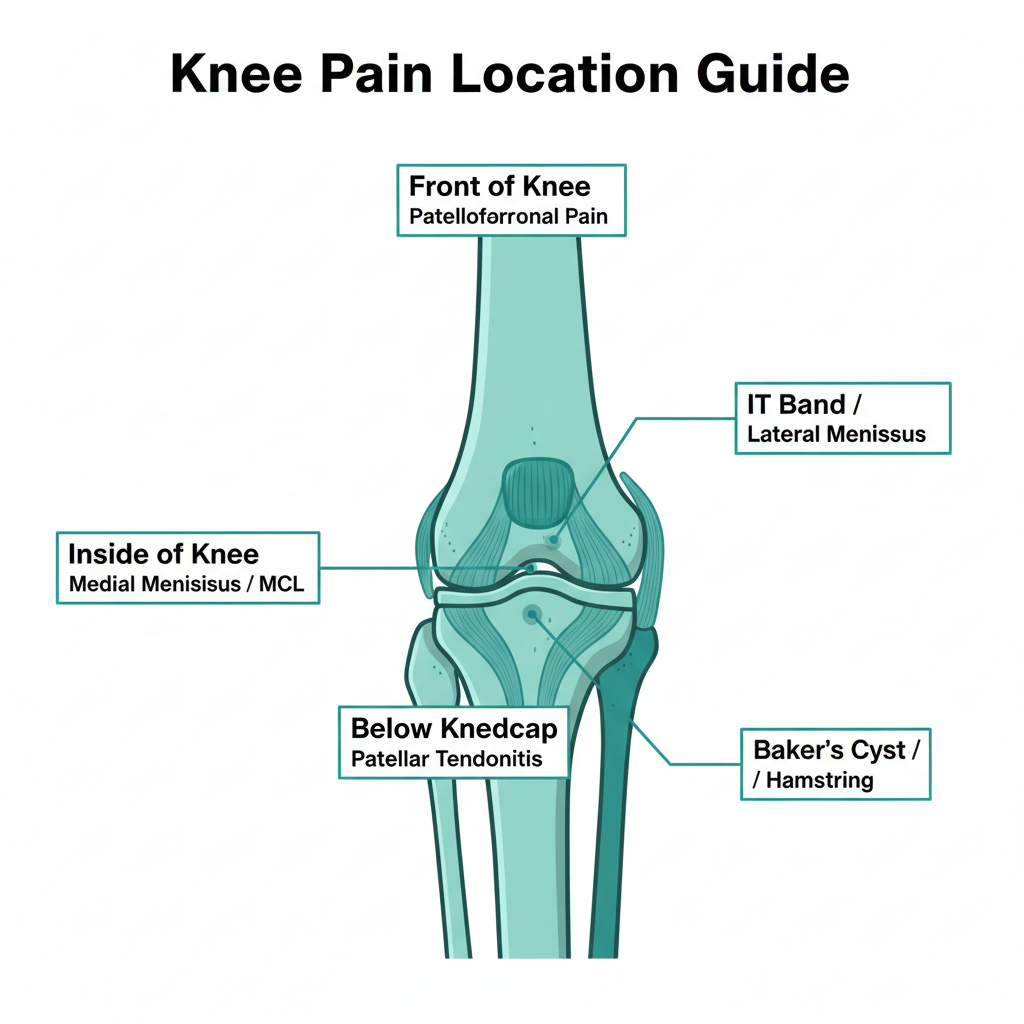
Pain location is the single most useful clue for narrowing down the cause of knee pain when bending. Use this guide to match your symptoms:
Front of the knee (around or behind the kneecap): Patellofemoral pain syndrome, patellar tendonitis, prepatellar bursitis, or chondromalacia. Learn more on our chondromalacia patella page.
Below the kneecap: Patellar tendonitis (jumper’s knee), Osgood-Schlatter disease in adolescents.
Inside of the knee (medial): Medial meniscus tear, MCL sprain, pes anserine bursitis.
Outside of the knee (lateral): IT band syndrome, lateral meniscus tear, lateral collateral ligament injury. See our IT band syndrome page for details.
Behind the knee: Baker’s cyst, hamstring tendonitis, posterior meniscus tear, popliteal tendon injury.
Deep inside the joint (hard to pinpoint): Cartilage damage, early osteoarthritis, loose bodies within the joint.
Swelling changes the clinical picture significantly. Rapid swelling within 2 hours of an injury suggests bleeding inside the joint (hemarthrosis), which typically means a ligament tear, fracture, or significant meniscus tear. Gradual swelling developing over 24 to 48 hours is more consistent with inflammation from a meniscus tear, bursitis, or arthritis flare.
If your knee pain when bending includes any of these signs, schedule an evaluation promptly:
Read our complete guide on how to tell if a knee injury is serious for a full symptom checklist.

Most patients who search “why does my knee hurt when I bend it” are trying to decide whether they need professional help. Understanding what actually happens during an evaluation removes the uncertainty.
At Sports Pain Management NYC, a typical knee pain evaluation with Dr. Melepura includes:
The entire evaluation takes 30 to 45 minutes. In many cases, Dr. Melepura can provide a diagnosis and begin treatment during the same visit. This is a key difference between seeing an interventional pain specialist and waiting weeks for an orthopedic surgery referral — the goal is to diagnose and treat, not to evaluate for surgery as a first step.
Treatment follows a clear progression based on diagnosis and severity. Most patients do not need surgery.
Structured physical therapy targeting quadriceps strengthening, hip stabilization, and movement mechanics resolves 70 to 80 percent of non-surgical knee pain cases. The program should be specific to the diagnosis — patellofemoral pain requires different exercises than a meniscus tear or IT band issue.
When home care and physical therapy are not sufficient, interventional pain treatments offer an effective middle ground between living with pain and surgery:
Most of these procedures take 15 to 30 minutes, are performed in-office using ultrasound or fluoroscopic guidance for precision, and require no downtime. Learn more on our knee injection treatments page.
Preventing knee pain when bending comes down to three fundamentals that apply whether you are a runner, lifter, cyclist, or weekend warrior in New York City:
For NYC-specific guidance on knee-friendly exercises and self-care protocols, visit our knee exercises page.
Meniscus tears produce mechanical symptoms like catching, clicking, locking, or a sharp pain at a specific angle during bending. Arthritis causes a more diffuse, grinding pain with morning stiffness that improves with gentle movement and worsens with prolonged activity. Meniscus tears are often unilateral (one knee), while arthritis frequently affects both knees. A physical exam and MRI provide definitive differentiation.
Keep moving with modifications. Current evidence shows that controlled movement promotes healing and prevents the muscle weakness that prolonged rest causes. Avoid the specific activity that triggers sharp pain, but continue low-impact movement like walking, swimming, or cycling. Complete immobilization is only appropriate for acute ligament injuries or fractures, and only for a limited period.
Mild overuse pain and minor strains often resolve within 1 to 3 weeks with activity modification and basic home care. However, pain that persists beyond 3 weeks, involves clicking or locking, or is getting progressively worse indicates a structural problem that is unlikely to resolve without treatment. Early intervention prevents a treatable condition from becoming a chronic one.
An interventional pain specialist focuses on diagnosing the pain source and treating it with targeted, minimally invasive procedures like image-guided injections, nerve blocks, and regenerative treatments. An orthopedic surgeon evaluates whether surgical repair or replacement is needed. Many knee conditions that were historically treated with surgery, including certain meniscus tears and early arthritis, now respond well to interventional approaches. Seeing a pain specialist first is often the faster and less invasive path.
At Sports Pain Management NYC, Dr. Melepura offers same-day and next-day appointments. Most patients receive a diagnosis during their first visit, including in-office diagnostic ultrasound when needed. MRI results are typically available within 48 to 72 hours if advanced imaging is indicated. The goal is a diagnosis and treatment plan within your first week, not months of waiting.
Going down stairs places the highest compressive force on the kneecap, up to 3.5 times your bodyweight compared to 2.5 times going up. This makes downstairs pain a hallmark of patellofemoral pain syndrome and chondromalacia, where the cartilage behind the kneecap is irritated. If going down stairs is your primary pain trigger, a focused quadriceps and hip strengthening program is the most effective first-line treatment.
If your knee hurts every time you bend or straighten it and home treatment is not making a difference, Dr. Melepura at Sports Pain Management NYC can identify the cause and start treatment, often during the same visit. Our Manhattan office offers same-day appointments, in-office diagnostic imaging, and the full range of non-surgical knee treatments. Schedule your evaluation here.

Febin Melepura, MD is a top rated, best in class interventional pain management doctor. He is a nationally recognized pain relief specialist and is among the top pain care doctors in New York City and the country. He is an award winning expert and contributor to a prominent media outlets.
Dr. Febin Melepura has been recognized for his thoughtful, thorough, modern approach to treating chronic pain and, among other accolades, has been named a “top pain management doctor in New York”, and one of “America’s Top Doctors™” for an advanced sports injury treatments.
